
Quick Answer: Most preschoolers are noisy, impulsive, and hard to redirect. ADHD is different in one specific way: the behavior appears across all settings, before age 12, persists for 6+ months, and significantly impairs daily functioning. Not just at home when tired. Everywhere. Always. Here are 7 questions that tell you whether what you're seeing is typical development or worth evaluating.*
I waited for him to grow out of it.
Everyone said he would. The pediatrician said most boys are like this at 3. His preschool teacher said he just needed more structure. My mother said I was too anxious.
So I waited. Three months. Six months. A year.
He didn't grow out of it.
He grew into a 5-year-old who had been asked to leave circle time every single day for a semester. Who had no close friends, not because he was unkind, but because he couldn't stop interrupting, couldn't wait his turn, couldn't stop moving even when he desperately wanted to join in. Who cried in the car every single afternoon. Not the exhausted cry of a tired kid. The specific cry of a child who knows something is wrong and doesn't understand why he can't fix it.
The problem wasn't that he was energetic.
The problem was that I didn't know the difference between energetic and struggling.
By the time you finish this article, you will.
This isn't my story. It belongs to a mom I know well — she lives two doors down. Real kid, real timeline, real outcome. I'm telling it with her permission because it's the one that made me understand what we're actually talking about when we say "he'll grow out of it."
First: 1 in 2 Preschoolers With ADHD Never Gets the Right Treatment. Here's Why That Starts With You.
Before any list of symptoms, one number that changes the context of everything that follows.
According to CHADD, roughly 1 in 2 preschoolers diagnosed with ADHD does not receive behavioral therapy — the treatment that research identifies as first-line for children under 6. Even more striking: 1 in 4 receives medication as the only treatment, despite clear AAP guidance that behavioral intervention should come first.
This isn't a medical failure. It's an awareness gap.
Most parents who reach the point of evaluation arrive late. After years of wondering. Months of being told to wait. The accumulated weight of feeling like they were somehow causing the behavior. The earlier a family understands what they're seeing and seeks an appropriate evaluation, the more options exist. And the more of a child's early developmental window is preserved.
You're reading this article. That already puts you ahead of the gap.
The full picture, by the numbers:
- 11.4% of children ages 3–17 in the US have been diagnosed with ADHD — approximately 7.1 million children (CDC, 2024)
- Only 2.4% of children ages 3–5 carry a formal diagnosis — a number that almost certainly undercounts the real prevalence
- ADHD prevalence in the preschool population ranges from 2% to 12.6% depending on the diagnostic method
- ADHD tantrums last an average of 20+ minutes vs. 1–5 minutes for neurotypical toddlers
- Boys are diagnosed twice as often as girls. Not because they have ADHD more often. Because their symptoms are more visible.
- More than 90% of children with ADHD will continue to have elevated symptoms into adulthood if untreated
That last number is the one worth sitting with. Not as a reason to panic. As a reason to pay attention now, while the window for early support is widest.
ADHD or Just Energetic? What's Actually Happening in the Brain (in Plain Language)
Before the test, a two-minute explanation of the neuroscience. Because the moment you understand what's happening in the brain, you stop asking "why can't they just listen?" and start asking the right questions.
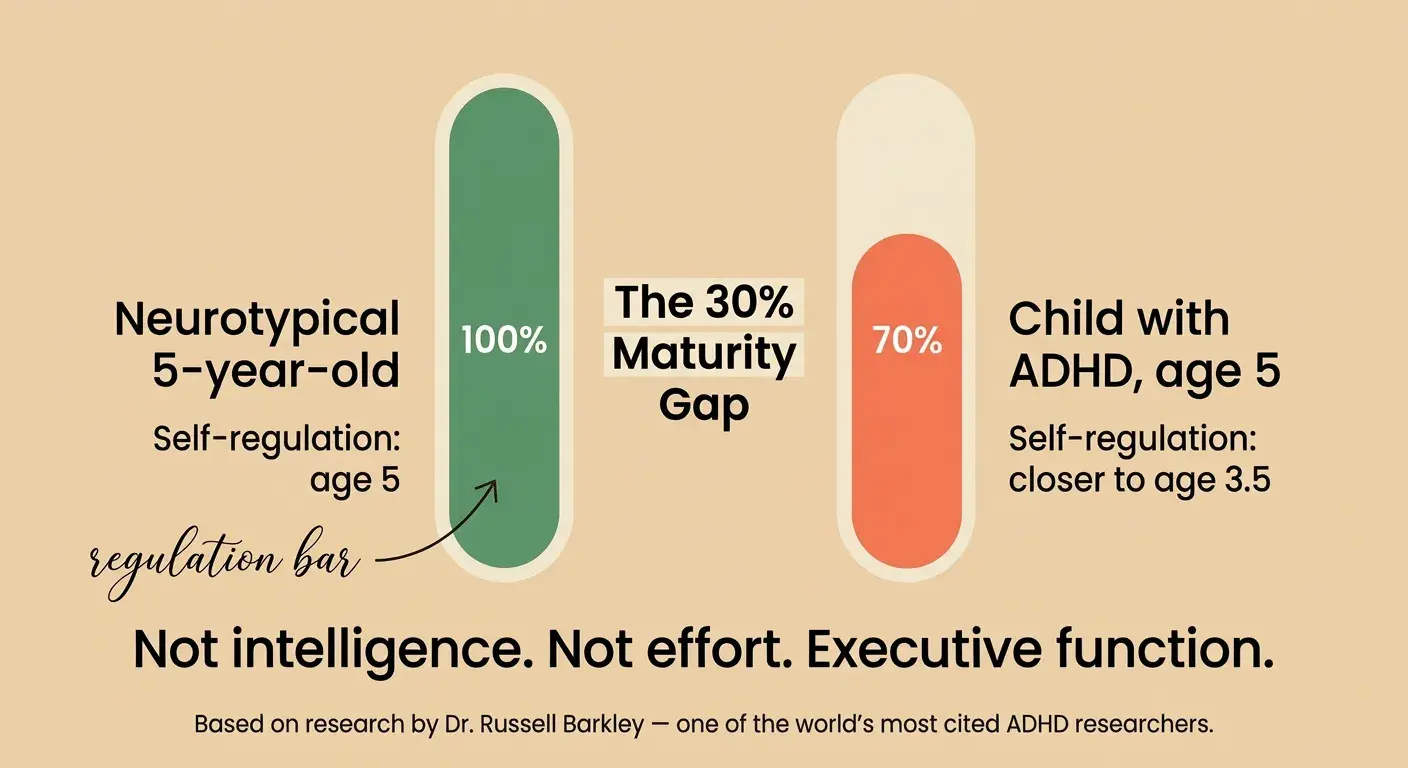
What the 30% Maturity Gap Means for Your Child — and for You
Dr. Russell Barkley, one of the most cited ADHD researchers in the world, identified a consistent pattern across dozens of studies: children with ADHD show a developmental delay of 25–41% in executive function relative to neurotypical peers. He rounded this to 30% for practical use with families.
In plain language: if your child is 5, their self-regulation system is operating closer to that of a 3.5-year-old.
Not their intelligence. Not their empathy. Not their creativity. Their capacity for impulse control, working memory, emotional regulation, and sustained attention.
This is why telling a child with ADHD to "just sit still" is roughly equivalent to asking someone with a broken leg to walk normally. The instruction isn't the problem. The architecture isn't ready yet.
Why "Just Try Harder" Is the Worst Thing You Can Say to an ADHD Brain
The prefrontal cortex develops more slowly in children with ADHD. This region communicates primarily via dopamine pathways, and in ADHD brains, that signaling is structurally different. The system responds less robustly to anticipated rewards and requires more immediate, concrete feedback loops to function.
"Trying harder" requires the very system that isn't working well to work harder. It's not a motivational problem. It's a neurological one.
Effort isn't the deficit. Architecture is.
The Dopamine Difference:
Why Delayed Rewards Don't Work
For most children, a sticker chart leading to a reward on Friday is meaningful. The brain assigns value to future outcomes, which creates behavioral motivation today.
For a child with ADHD, that pathway is significantly less efficient. The brain doesn't assign the same weight to Friday's reward on Monday morning. Which is why conventional behavior management systems — charts, deferred consequences, earning screen time for next week — frequently fail completely. Parents conclude their child "doesn't respond to incentives."
The child does respond to incentives. They respond to immediate ones. The system just needs to be built differently.

The 7-Point Test:
Early Signs of ADHD in a 3, 4, and 5-Year-Old
This is not a diagnostic tool. No article can diagnose ADHD. Proper evaluation requires a qualified clinician across multiple settings. What this test does: it helps you see whether what you're observing falls within typical development — or crosses enough thresholds to make a conversation with your pediatrician worth having.
The 7 Questions — With Thresholds That Actually Mean Something
Answer honestly based on what you observe across all settings. Not just at home during hard moments.

Question 1: Does the behavior appear in all settings — home, preschool, at grandparents', at birthday parties?
This is the single most important criterion. All young children have off days. ADHD behavior is pervasive. It shows up everywhere, not just when the child is tired or the parent is stressed. A child who only struggles at home is unlikely to meet ADHD criteria.
Threshold: Yes, teachers and other caregivers report similar observations independently.
Question 2: Has this been consistent for 6 months or longer?
ADHD is a persistent pattern, not a developmental phase. Many children go through high-activity phases, especially during major transitions. The DSM-5 requires symptom persistence for at least 6 months before an evaluation is meaningful.
Threshold: Yes, this has been the baseline behavior as far back as I can clearly remember.
Question 3: Is the behavior significantly more pronounced than in peers of the same age?
All 3-year-olds struggle to sit still. The question is whether your child is meaningfully beyond what other children the same age are doing. Teachers are especially useful here. They see dozens of children daily and have a calibrated baseline.
Threshold: Teachers or caregivers have specifically noted that this child is different from peers. Not just "active."
Question 4: Does it significantly impair daily functioning — friendships, learning, family life?
Activity level alone isn't ADHD. Impairment is the clinical threshold that separates ADHD from "spirited child." If the behavior is causing consistent problems with peer relationships, preschool participation, or family functioning, that's the signal.
Threshold: Yes. Rejected by peers, excluded from activities, learning participation consistently impaired, family life regularly disrupted.
Question 5: Is there impulsivity with risk — running into traffic, climbing without awareness of danger, acting before any thought?
Impulsivity in ADHD isn't just talking over people. It involves a genuine failure to connect action with consequence in the moment. The prefrontal cortex isn't flagging the danger before the body moves.
Threshold: Yes, and you've had genuine safety concerns that go beyond typical toddler testing.
Question 6: Does the child have difficulty sustaining attention even in preferred activities?
This is the most misunderstood criterion. Parents often say "but they can focus on screens for an hour." That's actually consistent with ADHD. Hyperfocus on highly stimulating activities is common. The question is whether they can sustain attention on tasks that require effort without constant novelty.
Threshold: Yes. Even with toys they love, they cycle through activities every 2–5 minutes unless the stimulation is extremely high.
Question 7: Were these patterns visible in infancy — difficult to soothe, low frustration tolerance from the very start, sleep problems from the beginning?
Research consistently shows that ADHD has early developmental roots. Infants who later develop ADHD are disproportionately described as difficult to soothe, highly reactive, and poor sleepers. Not definitive. But pattern data worth noting.
Threshold: Yes, this child has shown notably greater difficulty with regulation than is typical.
Scoring: 5 or more "yes" answers is a meaningful pattern worth discussing with your pediatrician. Not to receive a diagnosis, but to begin a proper evaluation process. Three to four: document and observe for 4–8 more weeks. Fewer than three: the pattern is more consistent with typical developmental variation.
ADHD vs. Normal Toddler Behavior:
Side-by-Side
Can You Diagnose ADHD at Age 3?
What the Research Actually Says
The official answer: ADHD can be clinically identified in children as young as 4, though most major guidelines recommend that formal diagnosis before age 4 be approached with significant caution.
At ages 3–4, the developmental range for self-regulation is extremely wide. What looks like ADHD at 3 resolves for many children by 4.5–5. The 30% maturity gap concept helps here — a child who is 30% behind at age 3 has more room for that gap to close compared to a child who is still 30% behind at age 6.
Don't wait to observe and document. Don't wait to talk to your pediatrician. But don't rush toward a formal diagnosis before age 4 unless impairment is severe.
The Sign Everyone Misses: Emotional Dysregulation Is the Earliest ADHD Marker
Here is the finding that almost no parenting article discusses. And that may be the most practically useful thing in this entire piece.
Emotional dysregulation — the inability to regulate emotional responses in proportion to their trigger — is not just a secondary feature of ADHD. Research shows it is one of the earliest detectable markers in preschool-age children who go on to meet ADHD criteria. It often appears before the classic hyperactivity and inattention symptoms are clearly differentiated from typical toddler behavior.
What this looks like in practice:
- Tantrums that are completely disproportionate to the trigger
- Extreme difficulty transitioning out of positive experiences — can't stop, even when they want to
- Rage responses that seem to come from nowhere and end just as suddenly
- Frustration that escalates instantly, with no middle step, from zero to complete overwhelm
Why ADHD Tantrums Last 20+ Minutes When Typical Ones Don't
The reason goes back to the dopamine and prefrontal cortex architecture. During an emotional episode, the regulation system that would normally modulate the response and bring the child back to baseline is the exact system that is structurally compromised in ADHD.
There is no internal braking mechanism working at full capacity. The episode runs until it runs out of fuel. Not until the child decides to stop.
The child isn't choosing this. There is simply nothing available to stop it with.
If you're seeing tantrums that consistently run 20+ minutes, appear with no warning, and end as suddenly as they began, across all settings, that pattern is more specific to ADHD than hyperactivity alone.
The Infant Signs Most Parents Don't Know Are ADHD Predictors
Looking back, many parents of children later diagnosed with ADHD describe a consistent pattern from the earliest months:
- Exceptionally difficult to soothe as a newborn
- Sleep problems more severe than peers from the beginning
- Extreme startle responses, high sensory reactivity
- Feeding difficulties tied to distractibility
- Inconsolable crying episodes without an identifiable cause
None of these are diagnostic. Many children with these patterns don't develop ADHD. But as context in a full evaluation, they are data points worth mentioning to your pediatrician.
What ADHD Looks Like in Girls — And Why It Goes Undiagnosed Until It's Too Late

If you're reading this for a daughter, this section is specifically for you.
Women with ADHD experience a nearly 4-year delay in receiving a diagnosis compared to men, despite equivalent symptom severity. Girls are diagnosed at significantly lower rates at every age. Not because they have ADHD less often. Because their symptom profile looks completely different.
What ADHD in a 5-Year-Old Girl Actually Looks Like
Boys with ADHD tend to present with the hyperactive-impulsive profile. The child who can't sit still, who runs into traffic, who talks over everyone. This is visible. Teachers notice. Referrals happen.
Girls more commonly present with the inattentive profile. Daydreaming. Forgetfulness. Disorganization. Social sensitivity rather than physical disruption. In a classroom, this child might sit quietly and appear to be listening. She isn't unreachable. She is somewhere else entirely. And no one refers her for evaluation because she isn't disturbing anyone.
Specific patterns in girls with ADHD:
- The "space cadet" — dreamy, often seems not to hear instructions, loses things constantly
- The "too sensitive" child — emotional intensity that adults attribute to personality, not neurobiology
- The social butterfly who can't keep friends — talks constantly, interrupts, doesn't read cues, but desperately wants connection
- The anxious one — secondary anxiety developing from years of trying harder than peers and still falling behind
- The good student who works twice as hard — masking through intense effort, which depletes by secondary school
Why Girls With ADHD Are Diagnosed 5–10 Years Later Than Boys
The masking starts early. Girls learn, from social cues and feedback and the pressure to be "good," to suppress the visible symptoms. They develop compensation strategies that are remarkably effective in structured preschool environments.
The cost: by the time the masking stops working — typically around puberty, when executive demands increase sharply — they've accumulated years of self-blame, anxiety, and an understanding of themselves as failing rather than as having an unaddressed neurological difference.
The earlier this pattern is recognized, the less of that accumulation a child has to undo.
The "Good Girl" Mask: How Girls Hide ADHD Symptoms
One practical test. Watch what happens at the end of a structured school day. Many girls with ADHD use enormous energy to hold things together in public. They come home and fall apart. Full meltdowns. Emotional flooding. Complete inability to do even simple tasks.
This isn't "bad behavior at home." It's a nervous system that has been compensating all day and has nothing left. The school day is evidence of how hard they're working. The afternoon is evidence of the cost.
5 ADHD Myths That Make Everything Harder (Including the Screen Time One)
Do Screens Cause ADHD? The Nuanced Answer
No. ADHD is a neurodevelopmental condition with 70–80% heritability. It is largely genetic in origin.
Here is the more precise picture: children with ADHD are disproportionately drawn to screens precisely because screens provide the kind of immediate, high-frequency reward feedback that the ADHD dopamine system responds to. Excessive passive screen time can amplify attention difficulties. But it doesn't create ADHD in a brain that wasn't already neurologically predisposed.
The pattern of screen over-use in a young child is more usefully read as a symptom than as a cause.
Does Sugar Make ADHD Worse?
What the Research Found
This is one of the most persistent myths in parenting culture. The research evidence for it is remarkably thin.
Multiple controlled studies, including double-blind designs where neither parents nor children knew whether sugar had been consumed, found no significant relationship between sugar intake and ADHD symptom severity. The perception that "sugar makes them worse" appears to be a combination of confirmation bias and the fact that high-sugar events are already high-stimulation environments.
Diet matters for ADHD in other ways — omega-3 fatty acids, iron levels, consistent meal timing are genuinely relevant to attention and regulation. But sugar as a primary driver of ADHD symptoms is not supported by evidence.
Is ADHD a Parenting Problem?
Here's the Genetics
No. ADHD is one of the most heritable conditions in psychiatry. Estimates range from 70–80% genetic contribution. Twin studies consistently show that identical twins are far more likely to both have ADHD than fraternal twins.
Parenting style can influence how well a child with ADHD is supported and helped to develop skills. It does not cause or create ADHD.
A parent who is struggling with a child with ADHD is not failing. They are managing something that would challenge anyone.
Are Children With ADHD Just Lazy?
The opposite is closer to the truth.
Research using neuroimaging consistently shows that the ADHD brain works harder on tasks requiring focused attention than a neurotypical brain. It recruits more neural resources to achieve results that come with less effort to typical peers. The brain's "resting state" network remains partially active during tasks where it should go quiet, creating constant internal noise that requires active effort to suppress.
Laziness implies an unwillingness to make effort. These children are often expending more effort than their peers. With less visible result.
Should Medication Be the First Step?
The American Academy of Pediatrics is unambiguous: for children under 6, behavior therapy is the recommended first-line treatment. Medication is considered only when behavioral intervention has been consistently implemented and has not produced sufficient improvement.
This isn't because medication is harmful. It's because the preschool brain responds less reliably to stimulant medication than older brains — approximately 50% response rate vs. 70% in school-age children — while behavioral intervention has a strong evidence base at this age with no side effect profile.
If medication is being offered before any behavioral intervention has been tried, that is not current AAP guidance. You can ask for a referral.
What to Do If You Suspect ADHD in Your Preschooler: A Step-by-Step Guide Before the Pediatrician Visit
Earlier engagement leads to better outcomes. Not because a preschooler needs to be diagnosed or medicated, but because earlier support — behavioral, environmental, structural — shapes the developmental trajectory in ways that matter.
Here's what to do before any clinical conversation.
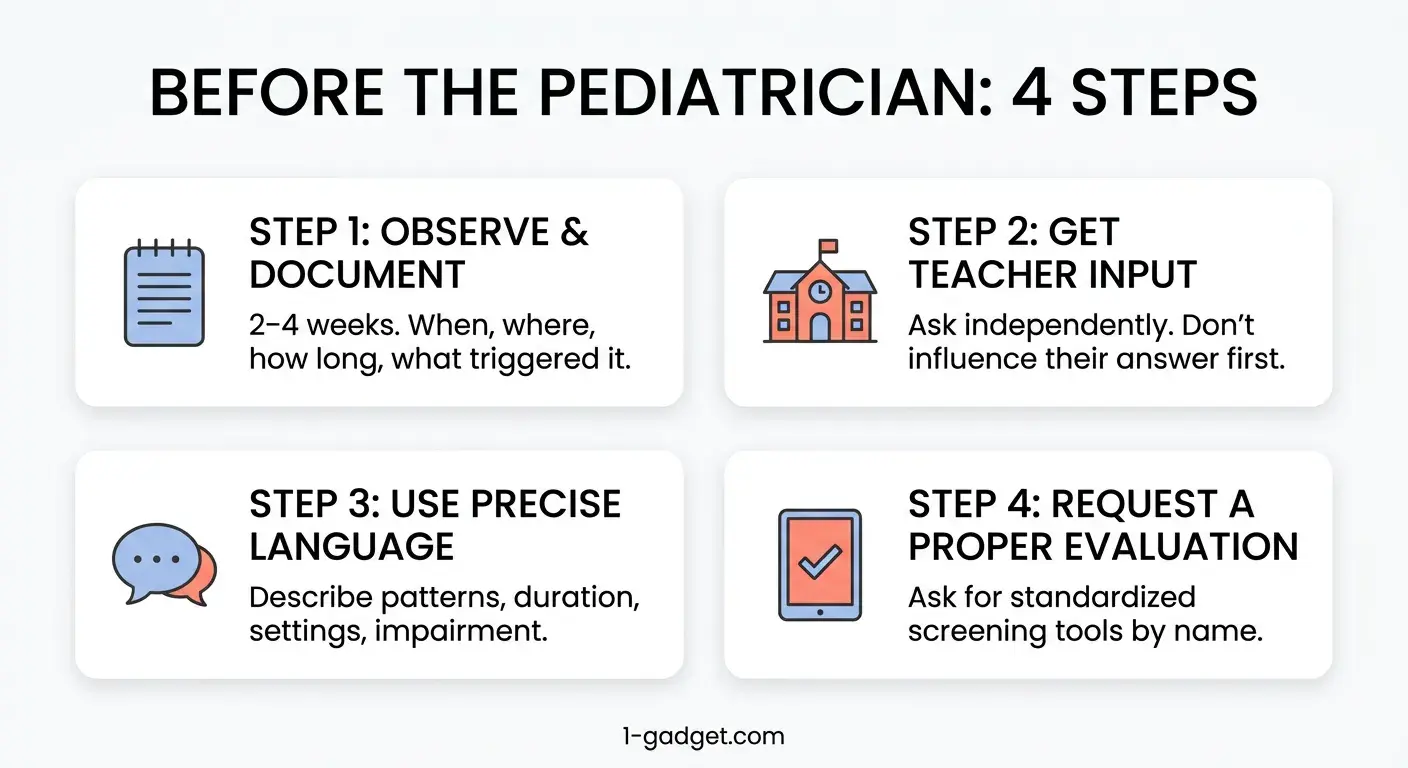
Step 1: The 2-Week Observation Log
Pediatricians and psychologists need behavioral data, not parental impressions. Keep a simple log for 2–4 weeks:
- When did the episode happen (time of day, what preceded it)
- Where (home, school, public, grandparents)
- How long it lasted
- What triggered it, or whether there was no clear trigger
- How it ended
- How frequently it happened that day, that week
Two weeks of this data gives a clinician more useful information than six months of parental worry.
Also: ask your child's preschool teacher to give you their observations independently, without you influencing them first. If their description matches yours without prompting, that's significant.
Step 2: What to Tell Your Pediatrician — Word for Word
Many parents walk into the pediatrician's office and say "he's really hyper" — and receive reassurance that all toddlers are hyper.
This is more precise:
"I've been tracking [name]'s behavior for the past [X] weeks across home and preschool settings. Both I and their teacher have independently described [specific patterns]. This has been consistent for [X] months and is significantly impacting [friendships / preschool participation / family functioning]. I'd like to understand whether a developmental evaluation is appropriate."
You can also specifically request a standardized screening tool — instruments like the Vanderbilt Assessment Scale or Conners Early Childhood Rating Scale are validated tools your pediatrician can use to structure the process.
Step 3: Rule Out the ADHD Mimics First
Several conditions can look like ADHD in preschoolers. A good evaluation rules them out before landing on an ADHD diagnosis:
- Sleep-disordered breathing — a child getting poor quality sleep is distractible, impulsive, and hyperactive. The single most common ADHD mimic.
- Anxiety — anxious children appear inattentive because they're occupied by worry, not by ADHD
- Sensory Processing Disorder — hyperreactivity to sensory input can drive behavioral patterns that look identical to ADHD
- Autism Spectrum — significant overlap in early presentations
- Iron deficiency or thyroid issues — medical causes that produce attention and behavior symptoms
- Language processing delays — a child who can't fully understand instructions appears non-compliant
Step 4: What a Proper ADHD Evaluation Actually Looks Like
In preschool-age children, a comprehensive evaluation typically includes:
- Structured clinical interview with parents covering developmental history
- Standardized rating scales completed independently by parents and teachers
- Direct observation of the child in multiple settings
- Ruling out medical causes (hearing, vision, blood work where indicated)
- Referral to a developmental pediatrician or child psychologist for neuropsychological testing where appropriate
What it is not: a 15-minute office visit and a symptom checklist. If that's what's offered, it is reasonable to request a referral to a developmental specialist.
How to Treat ADHD in Preschoolers: Behavior Therapy First, Medication Last — Here's the Research
Behavior Therapy First — Always
The AAP's Clinical Practice Guidelines are explicit: for children ages 4–5 with ADHD, behavior therapy is the recommended first-line treatment. For children under 4, parent training in behavior management is the first step before any formal diagnosis is even considered.
This is not play therapy or general counseling. It's specific, structured programs with robust outcome data:
- PCIT (Parent-Child Interaction Therapy) — highly effective for preschoolers with ADHD and co-occurring defiance
- Incredible Years — group-based program for parents and children with strong data for ages 3–8
- Triple P (Positive Parenting Program) — scalable, evidence-based, with significant ADHD-relevant outcomes
These three share the same mechanism: they teach parents to be the external regulation scaffold for a child whose internal regulation system isn't fully operational yet. Parents learn to provide the immediate, consistent feedback loops that the ADHD brain needs. And to do it in ways that build the child's own skills over time.
When Medication Is Considered
— and What the AAP Actually Says
For children ages 4–5, medication is considered only when behavioral intervention has been implemented consistently and the child's symptoms continue to cause significant impairment.
Stimulant medication shows a meaningful response in approximately 50% of preschoolers, compared to 70% in school-age children. Side effects — appetite suppression, sleep disruption, mood changes — occur at higher rates in young children.
For children under 4, the AAP recommends against stimulant medication except in unusual circumstances with specialist oversight.
If medication is being discussed for your preschooler, these are reasonable questions to ask:
- What behavioral interventions have been tried, for how long, and with what results?
- What is the monitoring schedule for side effects?
- What outcome measures will tell us whether this is working?
ADHD and Preschool:
How to Work With Teachers
What actually helps in a preschool setting:
- Visual schedules so the child can see what comes next; transitions named before they happen
- Seating near the teacher, away from high-distraction peers
- Frequent, brief tasks over long sustained ones
- Immediate, specific positive feedback. Not "good job" — but "you sat in circle time for three whole minutes. That was hard and you did it."
- Movement breaks built into the schedule, not offered as alternatives to participation
The single best thing you can do: share your observation log with the teacher. Ask them to share what they're seeing at school. A shared language between parent and teacher is one of the most powerful early interventions available
How to Support a Child With ADHD at Home: 4 Daily Principles That Actually Work
Principle 1: Immediate Feedback Over Delayed Rewards
Sticker charts that accumulate toward a Friday reward don't work for most children with ADHD. The dopamine system doesn't connect Monday's behavior to Friday's outcome with sufficient motivational weight.
What works: feedback that is immediate, specific, and visible. The moment a task is completed, something positive happens. A point earned. A physical token. A specific verbal acknowledgment. Not after three more tasks. Right now.
This is also why game structures work disproportionately well for children with ADHD. Games provide exactly what the ADHD brain needs: clear rules, immediate feedback, visible progress, a reward timed to the action.
The question most parents ask at this point: okay, but what does that actually look like on a Tuesday morning when we need shoes on in four minutes?
Here's one answer.

FirstGadget is built on exactly this architecture. When your child completes a real-world task — gets dressed, brushes teeth, puts on shoes — the app registers it in real time. Kevin the Fox's mission advances. Points appear immediately. The connection between action and reward happens in the moment the child's brain can actually process it.
This isn't gamification for its own sake. It's structuring the feedback loop to match the neurological architecture. The same principles that make behavioral therapy effective — immediate, consistent, visible positive consequences — applied to the routines that cause the most daily friction.
Transition moments that generate most household conflict become missions with immediate visible stakes. A parent stops being the enforcer. And the nervous system that struggles with delayed consequences suddenly has something it can work with.
Principle 2: Predictable Structure Is Medicine
For a child whose internal regulation system isn't fully operational, external structure does the regulating that the brain can't yet do alone.
Predictable sequences, visual schedules, consistent transitions. These aren't luxuries. They're the scaffolding.
When a child with ADHD knows exactly what comes after breakfast, and after getting dressed, and after shoes, the decision points that create friction largely disappear. Build the routine once. Visualize it. Make it the same every day. The investment pays back every single morning thereafter.
Principle 3: Movement Is Not the Problem. It's the Tool.
One of the most counterproductive responses to hyperactivity is removing movement as a consequence. "You can't go to the playground because you couldn't sit still."
Physical movement is both a symptom and a genuine regulatory tool. Research consistently shows that aerobic exercise improves attention and reduces ADHD symptom severity in children — not as character-building, but as a measurable neurobiological effect that temporarily elevates dopamine and norepinephrine.
The child who runs a lap around the yard before homework is not being rewarded for bad behavior. They're priming their brain for the cognitive task ahead.
Principle 4: Short Tasks, Clear Sequences, Visible Progress
Working memory in ADHD is genuinely impaired. The child is not ignoring your five-step instruction. They lost it after step two.
Build tasks in units of one or two steps. State them once. Use visual or physical cues rather than verbal instructions wherever possible. A picture of shoes next to the door is more reliable than "go put your shoes on" said for the fourth time.
Visible progress — a checkmark, a physical token, a task moved from "to do" to "done" — activates the same reward pathway that motivates completion. Small wins are not small. They are the entire architecture.
ADHD vs. Autism in Toddlers:
How to Tell the Difference
The confusion is understandable. The two conditions share significant surface-level overlap in preschool-age children, and they frequently co-occur — 30–50% of children with autism also have ADHD.
The most useful distinguishing question: does your child want to connect with peers but struggle to do so? (ADHD pattern.) Or are they relatively indifferent to peer connection altogether? (more characteristic of autism.)
These are not clean lines. A developmental evaluation that screens for both is the appropriate next step when there is meaningful overlap.
Your Questions, Answered
What are the earliest signs of ADHD in a 3-year-old?
The earliest and most consistently predictive sign is emotional dysregulation that is significantly beyond peers — tantrums that last much longer, frustration responses disproportionate to the trigger, difficulty calming even with parental support. Physical hyperactivity often follows. Emotional dysregulation usually comes first.
Can a preschooler be diagnosed with ADHD?
Yes, from age 4, with appropriate caution. The AAP acknowledges that reliable diagnosis is possible at 4–5 with a proper multi-setting evaluation. Before age 4, parent training in behavior management is recommended first.
Is my child hyperactive or just energetic?
Run the 7-point test. The core question: does the behavior appear in all settings, consistently, for 6+ months, and significantly impair functioning? Energetic children who are well-regulated can sit when needed, respond to consequences, and maintain peer relationships. ADHD is pervasive, not situational.
How do you test a toddler for ADHD?
There is no single test. A proper evaluation includes parent and teacher rating scales completed independently, a structured clinical interview, direct observation, and ruling out medical and developmental causes. Standardized tools like the Vanderbilt Assessment or Conners Early Childhood scales are used by clinicians.
Does ADHD get worse with age if untreated?
More than 90% of children with ADHD continue to have elevated symptoms into adulthood. It does not reliably "burn off." Untreated ADHD in childhood is associated with significantly poorer outcomes across education, relationships, employment, and physical health. The earlier support is put in place, the less that trajectory compounds.
What helps a child with ADHD focus?
Immediate feedback over delayed rewards, predictable structure, movement before demanding cognitive tasks, short tasks with clear sequences, and minimized environmental distractions. Behavioral therapy programs like PCIT and Incredible Years teach parents to implement these systematically.
Can screen time cause ADHD symptoms?
Screens don't cause ADHD. But children with ADHD are disproportionately drawn to screens because of the immediate reward structure. A child who cannot regulate away from screens may be showing a pattern consistent with ADHD, not a screen-caused one.
What foods help children with ADHD?
The best-supported factors are omega-3 fatty acids, adequate iron, consistent protein intake to stabilize blood sugar, and minimizing artificial additives where they appear to be individual triggers. No food treats ADHD. But nutritional foundations support everything else.
How is ADHD different from autism in toddlers?
Children with ADHD typically want peer connection and struggle to maintain it. Children with autism may be more indifferent to peer connection. Language is usually typical in ADHD and may be atypical in autism. Sensory reactivity is more systematic and pervasive in autism. Both can co-occur.
Should I medicate my preschooler for ADHD?
Not as a first step. For children under 6, the AAP recommends behavioral therapy first. If medication is being discussed before any behavioral intervention has been tried, ask for a referral to a developmental specialist.
Your Child Isn't Broken.
They're Wired Differently.
Here is what the research, the clinicians, and the parents on the other side of this all agree on.
The outcome for a child with ADHD is not determined by the diagnosis. It is shaped by what happens after the recognition. How quickly appropriate support is put in place. How the adults around the child understand and adapt to their neurology. And how the child learns to understand themselves.
A child who grows up being told they're lazy, difficult, and defiant develops a very different relationship to themselves than a child who grows up understanding that their brain works differently. Not worse. Differently. And knowing what it needs.
That difference starts with you. Right now. Before any diagnosis.
You are not looking for a label. You are looking for accurate information. The 7-point test won't diagnose your child. But it will give you a clearer map of what you're looking at. Which questions to ask. What to bring to the conversation with your pediatrician. And what to put in place at home while you navigate the rest.
The children who do best are the ones whose parents understood what was happening early enough to get ahead of the shame spiral.
Now you know what to look for.
Start with FirstGadget's morning and evening sequences this week. Structure and immediate feedback are the two most evidence-based, parent-available tools for supporting a child with ADHD before, during, and after any clinical process. Seven minutes to set up. Potentially transformative for the mornings that were costing everyone the most.
If your child's episodes look more like emotional overload than defiance — read our guide on tantrums vs. meltdowns. And if you're the one running on empty while managing all of this — the parental burnout guide is here. You are not alone in either.