
Quick answer: Picky eating peaks at age 2 and affects up to 60% of preschool children. Research shows it takes 8 to 15 exposures before a child accepts a new food. Most parents stop at 3 to 5 — often right before the shift happens. The single most counterproductive thing you can do at the table is apply pressure. Studies consistently show it increases mealtime conflict and entrenches the behavior you're trying to change.
The pasta tonight is wrong.
Not undercooked. Not burned. Same pasta as usual, same box, same brand. But tonight the shape is slightly different.
Dinner is over.
You stand in the kitchen looking at the untouched plate. You think about the article you read last week — the one about toddler nutrition and variety. The one that made you feel, once again, like you're doing this wrong.
You're not doing it wrong.
You're parenting a toddler in 2026, with three decades of contradictory advice in your pocket, a child whose brain is running a very specific developmental program right now, and very little guidance on what any of it means.
Here's what it means.
You Made a Second Dinner Last Night. And the Night Before. You're Not Alone.
59% of parents say they have a picky eater. 63% regularly cook a separate meal for their child. 57% have resorted to a bribe at some point — "just one bite and then you can have dessert." (Home Run Inn Picky Eating Report, 2024)
If that last number felt like a confession — it isn't. It's just a Tuesday.
The exhaustion here isn't only physical. It's the particular kind of drain that comes from caring deeply about something you can't control. You know nutrition matters. You're putting the broccoli on the plate every night. Watching it go untouched every night. Wondering what you're missing.
Here's what you're probably missing: one number. We'll get to it.
Why "just try it" backfires — every single time
When a child refuses food and a parent pushes, the child's nervous system registers the table as a conflict zone. The food on the plate becomes associated with pressure and tension — not with eating. Over time, that association deepens.
Not because the child is being difficult. Because that's how associative memory works in a developing brain.
Research published in PMC (PubMed Central, 2021) found that children who were pressured to eat showed greater, not fewer, mealtime conflicts over time. The American Academy of Pediatrics puts it plainly: "Pressuring kids to eat, or punishing them if they don't, can make them actively dislike foods they may otherwise like."
The harder you push, the more firmly the door closes.
That's not a parenting failure. It's biology.
The Evolutionary Reason Your Toddler Is Suspicious of Broccoli
Around age 2, a child who previously ate almost anything becomes deeply mistrustful of anything unfamiliar — anything green, anything touching something else on the plate, anything that arrived in a different shape than last Tuesday.
It feels like a step backward.
It isn't.
The growth slowdown nobody warned you about
In the first year of life, a baby's weight triples. The body is in overdrive, demanding fuel at a rate it will never match again.
Around 12 to 18 months, growth slows dramatically. The body needs significantly fewer calories — and the appetite follows. Many parents interpret this as their child suddenly refusing to eat. The child is eating precisely as much as their body requires.
The problem isn't the eating. It's the expectation built during year one.
This is documented by the American Academy of Pediatrics and explains a significant portion of what gets labeled picky eating in toddlers aged 1 to 3.
When food neophobia is actually a feature, not a bug
Food neophobia — the refusal to try unfamiliar foods — peaks between ages 2 and 6. Its evolutionary logic is simple: this is exactly when a child starts moving independently and can reach almost anything.
A brain that treats unknown objects as potentially dangerous is doing its job. The same instinct that kept our ancestors from eating unfamiliar berries shows up, in 2026, as a 3-year-old refusing mango they've never seen before.
Research in PMC (2024) estimates that food neophobia affects up to 59% of children aged 1 to 6. It has a genetic component. It is not a disorder. It tends to resolve as the child's world expands.
Knowing this doesn't make the second dinner less tiring. But it changes what you're actually solving for.
Is This Normal — or Something More?
The 4-Level Scale Every Parent Needs
Most picky eating content sits at one of two extremes: "It's totally normal, don't worry" or "These are warning signs of a serious disorder."
Neither is especially useful on its own.
What's missing is a spectrum. Because there are four meaningfully different things that can look identical at the dinner table — and each one needs a different response.
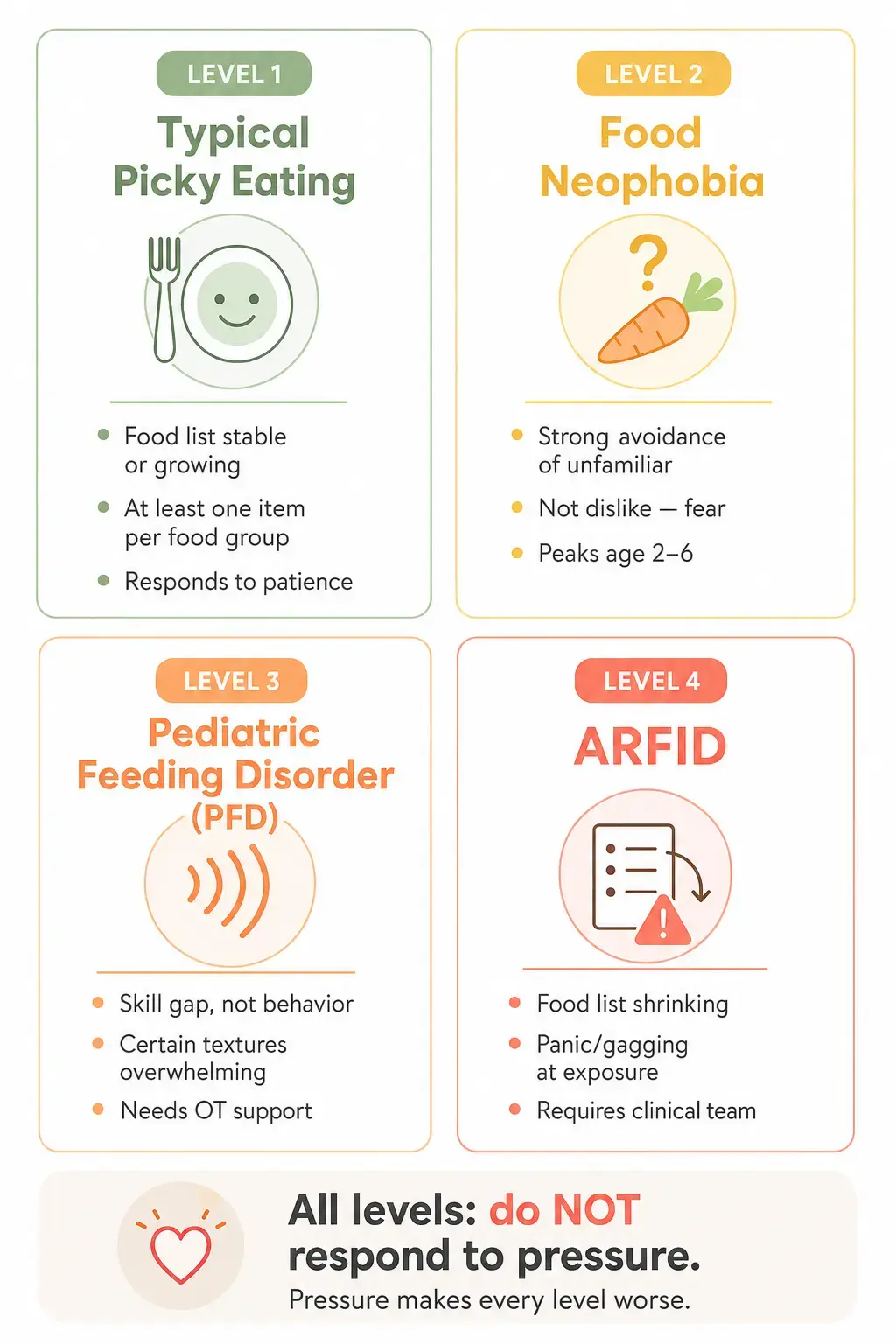
Level 1 — Typical picky eating (developmentally normal)
The child has preferences. Refuses certain textures or foods in phases. Accepts at least a few items from most food groups. Growth is on track. The list of accepted foods stays roughly stable or slowly expands.
This is the majority of toddlers aged 2 to 5.
Level 2 — Food neophobia (fear of the unfamiliar)
Strong, consistent resistance to anything new. Not dislike — avoidance. The child may refuse a food because of its color, its proximity to another food, or the fact that it looks slightly different than last time.
Peak window: ages 2 to 6. Responds well to repeated, pressure-free exposure over time.
Level 3 — Pediatric Feeding Disorder / PFD (a skill gap, not a behavior problem)
PFD involves a deficit in the physical or sensory skills of eating — oral motor coordination, sensory processing, swallowing mechanics. The child isn't refusing out of preference. Certain textures, temperatures, or consistencies are genuinely overwhelming to process.
Often seen in children who are premature, have developmental delays, or known sensory processing differences. Requires occupational therapy or a feeding specialist. A different dinner strategy won't reach this.
Level 4 — ARFID, Avoidant/Restrictive Food Intake Disorder (when professional support is non-negotiable)
Avoidant/Restrictive Food Intake Disorder is a DSM-5 diagnosis. The critical distinction from everything above: the list of accepted foods is actively shrinking. Not stable — shrinking. Exposure to non-accepted foods produces genuine panic, gagging, or vomiting.
Up to 15% of children may meet ARFID criteria (Eating Recovery Center, 2025). It requires a multidisciplinary clinical team.
Before You Try Any Strategy — Rule Out This First
Most picky eating guides skip this entirely.
A real subset of children who appear picky at the table are not being selective. They're uncomfortable. Every time they eat, something doesn't feel right — and they've found the only solution available to a 3-year-old: stop eating it.
When it's a physical problem wearing behavioral clothes
Acid reflux in young children doesn't always show as heartburn. It can appear as reluctance to eat, preference for small quantities, or avoidance of foods that worsen symptoms — acidic, fatty, or heavy textures. The child can't tell you their chest burns. They just stop eating those foods.
Constipation causes consistent, significant appetite suppression. Parents frequently misread this as selectivity. It isn't. It's a full digestive system with nowhere to go.
Eosinophilic esophagitis (EoE) is an immune-mediated condition causing esophageal inflammation. It presents as food refusal, slow eating, and frequent gagging — and gets missed for years.
One question before you change anything at the table
If mealtimes have been consistently distressing for more than two to three months, a conversation with your pediatrician before any strategy change is worth having. Ruling out physical causes first saves months of effort pointed in the wrong direction.
The Division of Responsibility in Feeding: The One Rule That Ends Mealtime Power Struggles
Registered dietitian and family therapist Ellyn Satter has spent decades studying how families feed children. Her Division of Responsibility in Feeding is the most rigorously studied approach to picky eating that exists.
It's also the one most parents have either never encountered — or encountered but underestimated.
The parent's job: what, when, and where
You decide what food is offered. When meals and snacks happen. Where the family eats.
That is the complete scope of your role.
The child's job: whether and how much
The child decides whether they eat what's offered. And how much.
Not "whether they eat everything." Whether they eat at all — and how much of what's available they choose to take.
This is the part that requires the most trust. Because it means tolerating the possibility that your child leaves the table having eaten very little — without offering an alternative, without commenting, without negotiating.
The counterintuitive outcome: children raised with this structure develop better self-regulation of hunger and fullness, show significantly less food-related anxiety, and expand their food acceptance more reliably over time.
What this looks like on a real Tuesday evening
You put dinner on the table. One or two things you know your child accepts. Whatever else you've cooked. You eat together.
No comments on what's being eaten or not eaten. No alternatives offered. The meal ends when it ends. The kitchen closes.
"This approach offers you a way out of power struggles, tantrums, and frustrations at eating times," Satter writes, "and allows you to focus on what really matters."
Uncomfortable at first.
Then, gradually, it isn't.
The 8–15 Exposures Rule — and Why You're Probably Quitting Right Before It Works
Here is the number that changes everything.
A systematic review of 21 randomized controlled trials (National Center for Biotechnology Information, 2019) shows that children typically need between 8 and 15 exposures to a new food before they accept it.
Most parents offer a food 3 to 5 times before deciding the child doesn't like it and removing it permanently from the rotation.
The math is the entire problem.
But here's the piece that makes it genuinely painful: the research also found that progress from those early exposures is often happening — measurably, objectively — but invisible to the parent. The child's tolerance for the food is shifting before any eating occurs. Parents who stopped at try number 5 were frequently stopping at the exact moment the door was beginning to open.
Why try #4 feels like the final answer — and isn't
Repeated refusal looks identical whether it's the 3rd exposure or the 12th. There's no signal that says "this is working." Absence of visible progress and presence of invisible progress feel the same from the outside.
The only reliable strategy is to keep going — not because it always feels productive, but because the data says it is.
The silent plate
Put the new food on the plate. Say nothing about it. Don't encourage, don't comment, don't watch to see if it gets touched.
No "just one bite." No "you loved this last week." No "the bunny wants you to eat the peas."
Just presence.
If it goes untouched — fine. That's exposure number four. Or eight. The clock is still running.

From "I Won't Touch It" to "I'll Try It":
6 Methods With the Science Behind Each
1. Food bridges — from known to unknown via texture and color
The child accepts mashed sweet potato. Sweet potato is orange, soft, slightly sweet. So is butternut squash. So is carrot purée. So is pumpkin.
You're not introducing a new food. You're walking a bridge that already exists.
Bridge from what's accepted by matching texture first, then color, then flavor. The AAP (American Academy of Pediatrics) supports food bridging as one of the most effective strategies for expanding a limited repertoire without triggering rejection.
2. Food chaining — the slow lane
Move one attribute at a time.
Cucumber slices → cucumber with dip → carrot sticks with dip → raw carrot → steamed carrot → carrot in soup.
Each step is close enough to the previous that resistance is minimal. Eventually the destination is a food the child once refused entirely. Neither of you noticed the journey.
3. The "no thank you bowl"
A small bowl placed beside the plate. Unwanted food goes there — the child isn't required to eat it, only to move it.
The food stays present (exposure continues). The child has agency. The parent is out of the equation. No one is watching. No one is waiting.
4. Sensory play outside the meal
For children with sensory sensitivity, the resistance starts before the fork. The smell. The appearance. The possibility of touching it.
The rules away from the table are different. There's no plate. No expectation. Nobody watching what gets touched and what doesn't.
One parent described watching her 2-year-old eat raw onion and crumbled sheep's cheese. At dinner, he refused both every time. While helping make a salad, he ate them standing at the counter, piece by piece, with his hands, before they ever reached the bowl. Nobody offered them. Nobody watched. He just ate them.
The foods that never survive a dinner disappear during the preparation. Raw onion. Crumbled feta. A piece of cucumber. The child has no idea they're doing something they "don't like." They're just cooking.
Contact without expectation lowers the barrier more reliably than contact with pressure ever could.
5. Structured kitchen hours
One of the most underrated strategies — and one of the most effective.
When food is available at any time, a child who eats a cracker at 4:30 PM arrives at dinner with a diminished appetite. The parent reads the dinner refusal as pickiness. It's satiation timing.
Meals at predictable times, snacks with clear windows, kitchen closed between them: the child arrives at the table hungry. Hunger is the single most reliable predictor of food acceptance.
6. The 5-to-1 praise ratio
Borrowed from feeding therapy for children with autism — and useful for every child who feels observed at the table.
For every one moment of concern or correction ("you're not eating," "just try it"), aim for five moments of neutral or positive connection. About anything. What happened at the park. What the dog is doing. What color that cup is.
When the table feels safe rather than evaluative, eating behavior consistently improves. The child eats better when no one is watching them eat.
The Mealtime Mistake 57% of Parents Make — and the Fix That Feels Backward
More than half of parents have used dessert as leverage: "Eat your broccoli and you can have ice cream."
The logic is reasonable. The outcome isn't.
When dessert is the reward for enduring a less-preferred food, two things happen simultaneously. The less-preferred food is coded as the obstacle — the tax, the unpleasant thing you endure to get to the good part. The dessert is coded as the prize — the thing that's worth tolerating discomfort for.
Over time, that architecture deepens. The broccoli becomes more aversive. The dessert becomes more desirable. The gap between them widens, every dinner, a little more.
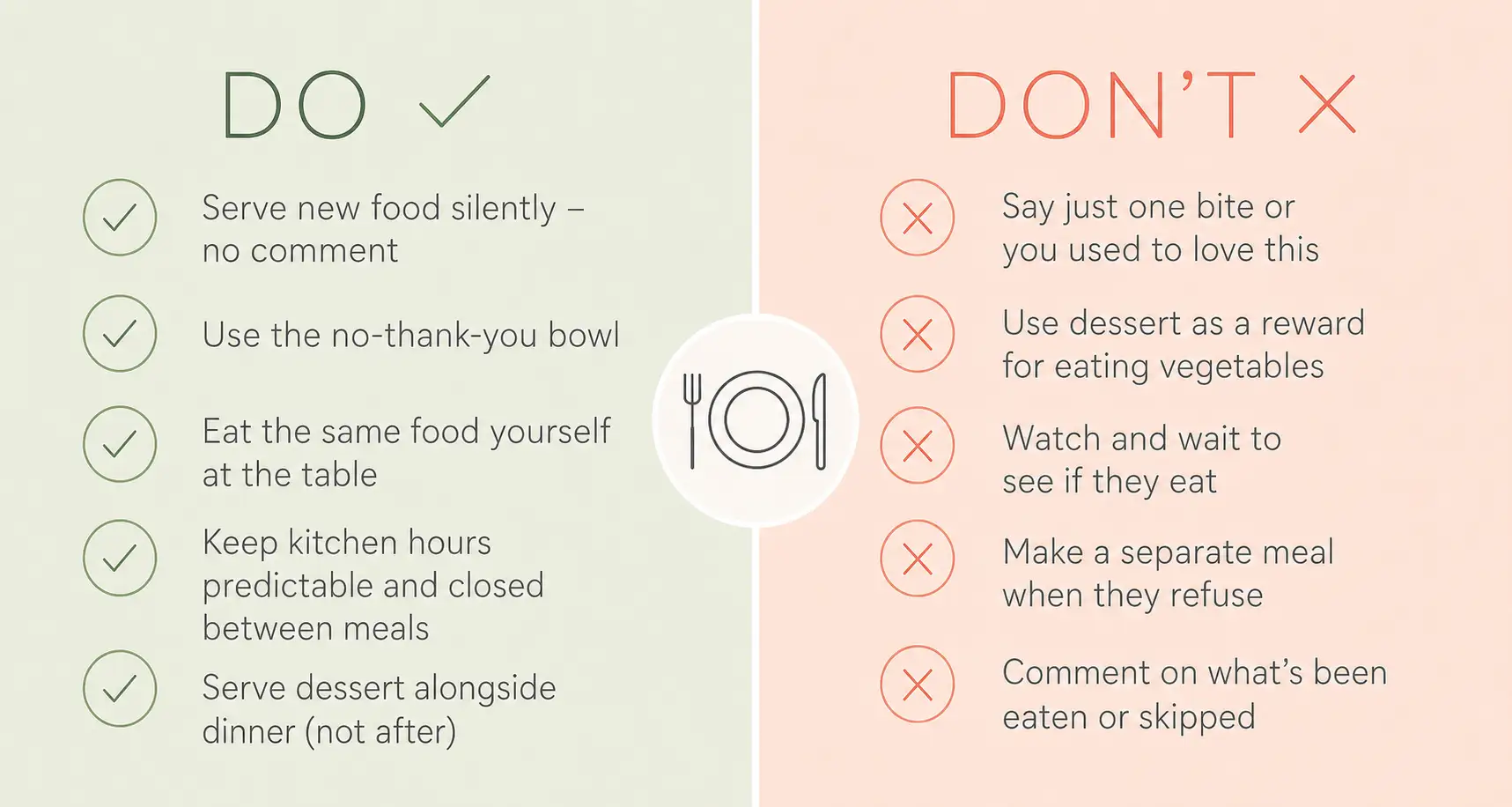
Serve dessert with dinner
Practitioners in pediatric feeding therapy consistently recommend serving dessert alongside the meal — not after. It sits on the plate from the beginning. The child can eat it at any point.
The result: dessert loses its status as a reward. It becomes just another thing on the plate — neither forbidden nor earned. Children raised with this structure show less dessert fixation, not more.
It's not a free-for-all. It's removing the architecture of control that creates the problem in the first place.
Is Picky Eating a Sign of Autism or ADHD? The Honest Answer
This is the question parents search at 11 PM. It deserves a direct answer — not a disclaimer-heavy non-answer.
The autism connection
Children with autism spectrum disorder are five times more likely to have significant feeding difficulties than neurotypical children. Research by Chistol et al. (Boston University, 2018) found atypical oral sensory sensitivity in 64% of children with ASD (Autism Spectrum Disorder), compared to 7% of neurotypical children.
In ASD, food selectivity tends to be more rigid, more tied to specific sensory properties — texture, temperature, color, packaging design — and less responsive to standard exposure strategies alone. Occupational therapy and speech-language pathology are typically needed alongside any behavioral approach.
The ADHD connection
ADHD looks different at the table. The issue is less about food refusal and more about the structure of eating: difficulty sitting for a full meal, impulsive behavior during eating, and appetite suppression that can be significant for children on stimulant medication.
Some children with ADHD also struggle to recognize hunger and fullness — a dysregulation of the same interoceptive system that medication affects.
What this means for you
Selective eating alone is not a diagnostic indicator of either condition. If picky eating is accompanied by other developmental differences — in social communication, attention, sensory responses, or emotional regulation — that conversation belongs with your pediatrician.
Picky eating without those co-occurring patterns is, in the vast majority of cases, a phase.
Red Flags: When to Stop Strategizing and Call Someone
Most picky eating does not require clinical intervention.
Some does — and the timing matters.
Speak with your pediatrician if:
- The list of accepted foods is shrinking, not stable
- The child accepts fewer than 20 foods total
- Gagging or vomiting occurs at the smell or sight of a non-accepted food
- At least one entire food group is absent
- Weight gain has stalled or growth is not tracking on the expected curve
- Mealtimes cause significant, consistent distress — for the child, not just for you
- The child avoids birthday parties, school lunches, or any eating in social settings
Who to call:
- Pediatrician first — rule out GI causes, assess growth, get a referral if indicated
- Occupational therapist — for sensory-based avoidance or oral motor challenges
- Speech-language pathologist — for difficulty chewing, swallowing, or food management in the mouth
- Registered dietitian — for nutritional assessment and supplementation during an active period of restriction

Why Every Feeding Therapist Starts With the Same Thing — and It's Not a Strategy
Ask any occupational therapist or feeding specialist what they do first, before introducing any technique.
The answer is always the same.
They build a routine.
Not because routine is the whole answer. Because without it, no strategy works. A child whose day is unpredictable arrives at the table with a nervous system already on alert — scanning for the next unexpected thing, spending cognitive resources on low-grade vigilance rather than openness. In that state, a new food on the plate isn't an invitation. It's another variable.
Predictability changes that. Meals at consistent times, in a familiar place, following a familiar sequence: the table stops being an event and becomes just part of the day. Unremarkable. Safe. A nervous system at rest is a nervous system capable of new experience — including, eventually, new food.
This is the foundation every feeding therapist lays before anything else.
What that looks like from the inside of a real morning
Wake up. Get dressed. Brush teeth. Sit down for breakfast. These steps happen in the same order, at the same time, every day.
The child stops bracing for what's next — because they already know what's next. And something shifts, almost imperceptibly, over weeks: mealtimes become less fraught. Not because the food changed. Because the context did.
First Gadget works inside exactly this kind of rhythm. When a child completes each step of their real-world morning — gets dressed, brushes teeth, sits down for breakfast — the app registers it in real time. Kevin the Fox's mission advances. Something happens immediately, visibly, as a direct result of what the child just did.
The structure that feeding therapists spend weeks building, a family can start reinforcing today. Consistently. Without the child needing to understand why. The routine becomes its own reward — and the table, quietly, becomes a safer place.

Frequently Asked Questions
About what's normal:
Will my picky eater grow out of it?
Most children do. Picky eating peaks around age 2 and decreases significantly by age 5 to 6. The exception: if the list of accepted foods is actively shrinking rather than stable or slowly growing — that's a conversation for your pediatrician, not continued waiting.
How many times should I offer a new food before I give up?
Between 8 and 15 times, according to a systematic review of 21 clinical trials (NCBI, 2019). Offer without pressure, without comment, without watching to see what happens. And accept that the progress is often invisible until it suddenly isn't.
What is the 80/20 rule for toddlers at mealtime?
Approximately 80% familiar and accepted foods alongside 20% less familiar or new foods at any given meal. The child isn't overwhelmed. The exposure still happens. Both things are true at once.
About the strategies:
What is the Division of Responsibility in feeding?
A framework developed by dietitian Ellyn Satter: parents decide what food is offered, when meals occur, and where the family eats. Children decide whether they eat and how much. Removing adult control over those last two variables consistently reduces power struggles and improves long-term outcomes.
What is the "no thank you bowl"?
A small bowl beside the child's plate. Unwanted food goes there — the child isn't required to eat it, only to move it. The food stays present for continued exposure without sitting on the child's main plate as a source of conflict.
Should I force my child to eat?
No. Research is consistent: pressure increases mealtime conflict, creates negative food associations, and entrenches the patterns you're trying to change. The AAP recommends offering food without pressure — the parent's job is to provide, the child's job is to decide.
About when to get help:
Is picky eating a sign of autism or ADHD?
Selective eating alone is not a diagnostic criterion for either. Children with ASD are significantly more likely to have feeding difficulties, but the inverse is not true — most picky eaters don't have ASD. If picky eating is accompanied by other developmental differences, speak with your pediatrician.
What is ARFID?
Avoidant/Restrictive Food Intake Disorder is a DSM-5 clinical diagnosis — not extreme pickiness, not a phase. Key signs: the accepted food list is shrinking, gagging or panic occurs at exposure to non-accepted foods, growth is affected, or a whole food group is absent. Professional evaluation is needed.
When should I stop trying strategies on my own and call someone?
When the food list is shrinking. When there's gagging or vomiting at the sight or smell of food. When growth has stalled. When fewer than 20 foods are accepted. When mealtimes cause significant distress for the child — not just frustration for you. These are signals for a professional, not a new strategy.

Your Parenting Co-Pilot
Less talk, more action. Turn daily routines into fun missions kids actually want to finish.
Available on iOS & Android